Please find the link below to his winning abstract as published in the Heart Lung and Circulation Journal, August 2022.

Please find the link below to his winning abstract as published in the Heart Lung and Circulation Journal, August 2022.
Summary by Dr Scott McAlister and Prof Alexandra Barratt
As published in The Lancet July 2022.
When we think of carbon (CO2) emissions we don’t often think of healthcare, yet healthcare in Australia is responsible for approximately 7% of national emissions. Approximately 30% of these emissions come from building energy, with most of the rest coming from medical products and processes, such as medical tests, devices and interventions. Carbon footprintingof products and processes involves quantifying emissions from all phases of a product’s life cycle, including extracting raw materials such as ore or gas, manufacturing, use, and then disposal such as through landfill or recycling.
Recent Australian carbon footprinting has been done for pathology testing, intensive care, anaesthesia, and diagnostic imaging. The imaging study showed that one MRI scan has a carbon footprint of 17.5kg CO₂ equivalents (CO2e), which is the same as driving a car 145km, while one CT scan has a footprint of 9.2kg CO₂e, or driving 76km. These are much higher than X-rays (0.76kg CO₂e, 6km) and ultrasound (0.53kg CO₂e, 4km). Reducing imaging or using lower carbon modalities reduces emissions.
One hidden area for healthcare is individuals’ travel for conferences. A return business class flight from Australia to the USA results in approximately 12 tonnes CO2e. By contrast, our individual annual carbon budget in 2030 to keep the world below 1.5°warming will be 2.2 tonnes CO2e.
Authors: McAllister S. et al; https://doi.org/10.1016/j.lanwpc.2022.100459
Explanation:

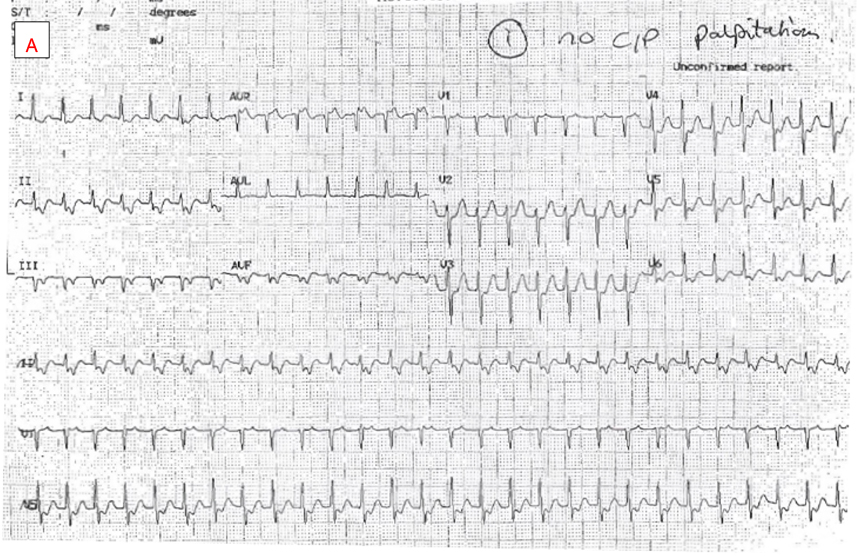
Panel A displays a short RP narrow complex tachycardia at a rate of approximately 160bpm. This is a supraventricular tachycardia (SVT). P waves can best be appreciated in the inferior limb leads, aVR and V1. There is a 1:1 RP relationship with the P wave falling in the first half of the RR cycle (short RP).
The P wave configuration is deeply negative in inferior limb leads and positive in aVR. It is isoelectric in the first half of V1 before becoming positive in the second half. This morphology is characteristic of a posteroseptal origin of atrial activation but is not diagnostic of tachycardia mechanism. It does however exclude option e) inappropriate sinus tachycardia, because this P wave configuration is inconsistent with a sinus origin of activation.
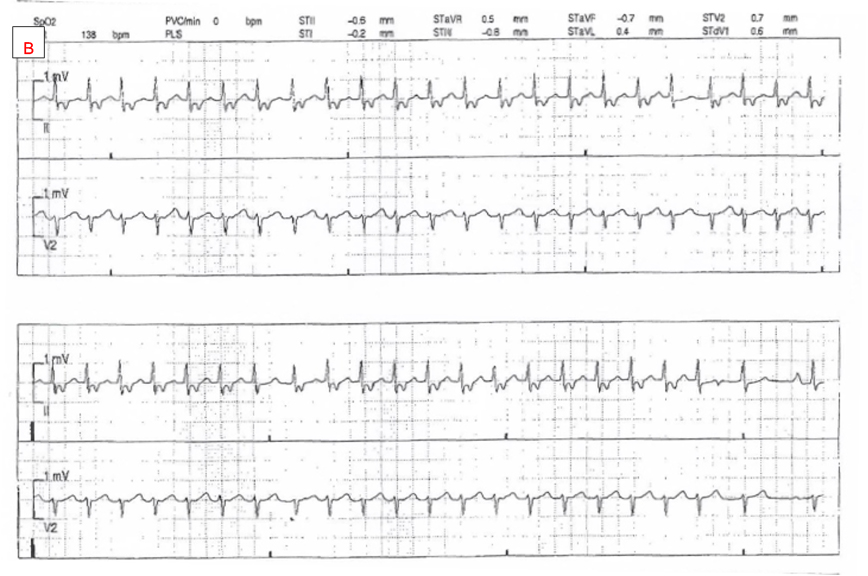
Panel B shows the rate of SVT has slowed to approximately 140bpm. All 12 leads are no longer available for P wave morphology analysis but the P wave appears unchanged in lead II. Notice that the RP interval is unchanged despite the slower tachycardia rate. Towards the end of the panel, we see a cycle where there is a dropped P wave (purple circle in between red arrows highlighting P waves). This phenomenon is seen again further along in the bottom of the panel. Tachycardia continues without reset despite the dropped P wave. This implies that atrial depolarization is not an obligate component of the tachycardia mechanism and thus option a) orthodromic AV reentry tachycardia can be excluded. This is because orthodromic AV reentry is due to the presence of a large loop circuit comprised of AV node, His-Purkinje system, ventricular myocardium, retrograde conduction to the atrium via an AV bypass tract, atrial myocardium, and then finally, the AV node again. Tachycardia is interrupted if any of these structures fail to depolarize. The dropped P waves seen here exclude orthodromic reentry because tachycardia continues at the same rate and is unaffected by the lack of atrial depolarization.
Additionally, it is readily apparent that with the dropped P waves the overall atrial rate is now lower than the ventricular rate. Consequently, the atrium cannot be driving this narrow complex tachycardia, hence options c) focal atrial tachycardia, and d) slow atrial flutter, can be excluded.
This leaves the correct answer as b) AV nodal reentrant tachycardia (AVNRT).
AVNRT is the most common form of SVT and is caused by reentrant excitation around perinodal transitional zone tissue. Neither atrial nor ventricular myocardium is required for ongoing AVNRT. While conduction block to the ventricle is commonly seen during AVNRT, block to the atrium is rarer. When conduction block to the atrium is seen during a narrow complex tachycardia however, it is very useful as it excludes most other common SVT mechanisms.
Provided by A/Prof Haris M. Haqqani – ECG of the Month – August 2022
Authors: Fang Shawn Foo, MBChB; Mildred Lee, MSc; Katrina K. Poppe, PhD; Geoffrey C. Clare, MBChB; Martin K. Stiles, PhD; Andrew Gavin, MBChB; Matthew Webber, MBChB; Rod Jackson, PhD; Andrew J. Kerr, MD;
Published in Heart Lung and Circulation 20 August 2022 with summary below by Dr Shawn Foo and A/Prof Martin Stiles.
Patients with heart failure and reduced ejection fraction are recommended to receive guideline directed medical therapy (GDMT). Many of these patients will also receive an ICD. This prompted Foo et al to look at almost 1700 ICD patients in New Zealand and, using prescribing records, determine which of these patients were receiving such medications at implant and one year later, and whether target doses were achieved. The specific classes of medication assessed were:
1. ACEi/ARB/ARNI
2. Beta blockers
3. Aldosterone antagonists
Note that the study period of 2009-2018 pre-dated the use of SGLT2 inhibitors.
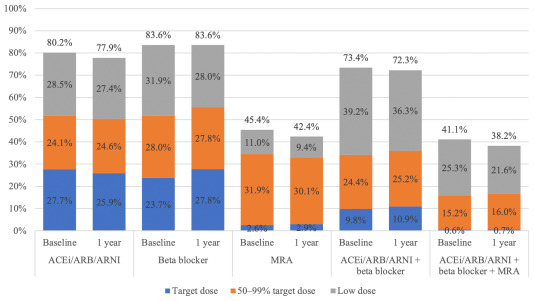
Foo found that although 80% of patients received ACEi/ARB/ARNI, 84% beta blockers and 45% aldosterone antagonists, a dose ≥50% of recommended target dose (based on international guidelines) was achieved in only 52%, 52% and 35%, respectively. In fact, just 16% of patients received ≥50% of the target dose of all three medication classes.
For the >98% of ICD recipients who were alive at one year, the proportions of patients dispensed each class of medication remained largely unchanged. In fact, no matter the class of medication, the vast majority (67-81%) of patients had no change to their medication dose between implant and one year later.
This data is important as it captures an entire nation through its national database and demonstrates the inertia of heart failure therapy. This group of ambulatory heart failure patients would likely benefit from a more intensive up-titration of medication doses to ensurethat the (now four) classes of GDMT were all prescribed, where appropriate.
Some of the patients in this cohort would have been at maximally-tolerated doses yet not achieved ≥50% of the recommended target dose due to limitations of (e.g.) low blood pressure or kidney function, but there is clearly room for improvement. Perhaps a greater integrated response from ICD clinics and heart failure services would improve the numbers of patients at target dose, translating to improved outcomes in such endpoints as hospitalisations and mortality. In fact, some have argued that repeating the primary prophylactic ICD trials in today’s era of four-agent heart failure therapy might demonstratelack of benefit for ICDs over modern medical therapy. This study suggests that, until we do better in replicating the doses achieved in pivotal trials, medical therapy for heart failure in practice does not match ‘gold-standard’ GDMT of the trials.
Guideline-directed medical therapy for heart failure in patients before and after receiving primary prevention ICD implant 2009-2018.
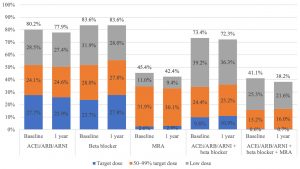
Abbreviations: ACEi, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor neprilysin inhibitors; ICD, implantable cardioverter defibrillator; MRA, mineralocorticoid receptor antagonists.
Published: August 20, 2022. DOI:https://doi.org/10.1016/j.hlc.2022.06.691

The Therapeutic Goods Administration (TGA) is seeking applications from professionals with expertise in relevant medical or scientific fields or consumer health issues to support their statutory advisory committees. These include:
Read more about the committee roles here.
Applications close at 11.30pm (AEST) this Sunday 4 September 2022.

CSANZ will be presenting a Daily Highlights session at the ESC Congress on Saturday, 27 August. The session will be hosted by Stephen Nicholls, Will Parsonage, Julie Redfern and Elizabeth Paratz.
If you are in Barcelona, you can attend the session at the Global Stage in the Global Community area at 10.15am.
For those of us back home in Australia and New Zealand, the session will be available to watch online on the Global Community dedicated section of the ESC Congress platform.
The restrictive access will enable you to enter these areas on the congress digital platform:
Research Gateway – abstracts and clinical cases. Comment, share and like on your favourites. Open from 22 August with all the Moderated ePosters, complemented with oral abstracts and clinical cases after the sessions and until 12 September.
Global Community – connect with your National Cardiac Society to network, discuss the science in a local context, and catch up with colleagues. Open from 22 August to 12 September.
Click this link to get your complimentary restricted access.
For full access to ESC Congress, registration is required as usual. Click here.