Explanation:

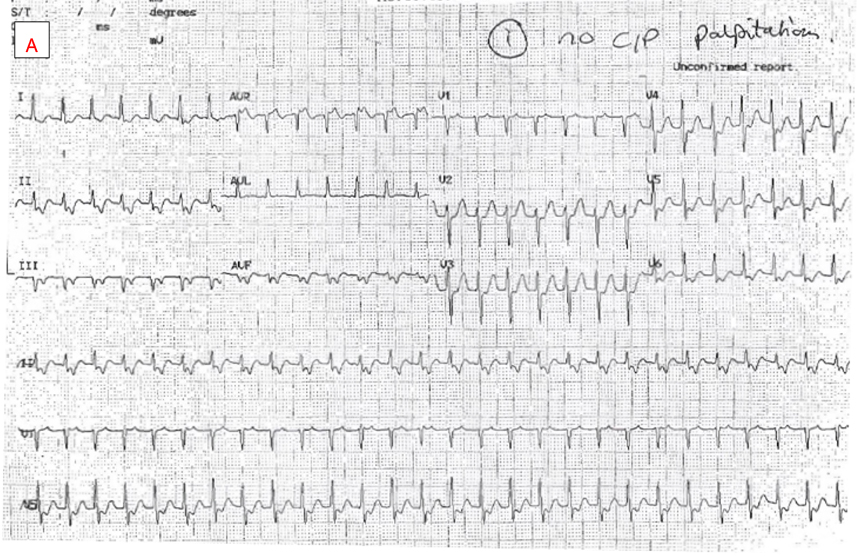
Panel A displays a short RP narrow complex tachycardia at a rate of approximately 160bpm. This is a supraventricular tachycardia (SVT). P waves can best be appreciated in the inferior limb leads, aVR and V1. There is a 1:1 RP relationship with the P wave falling in the first half of the RR cycle (short RP).
The P wave configuration is deeply negative in inferior limb leads and positive in aVR. It is isoelectric in the first half of V1 before becoming positive in the second half. This morphology is characteristic of a posteroseptal origin of atrial activation but is not diagnostic of tachycardia mechanism. It does however exclude option e) inappropriate sinus tachycardia, because this P wave configuration is inconsistent with a sinus origin of activation.
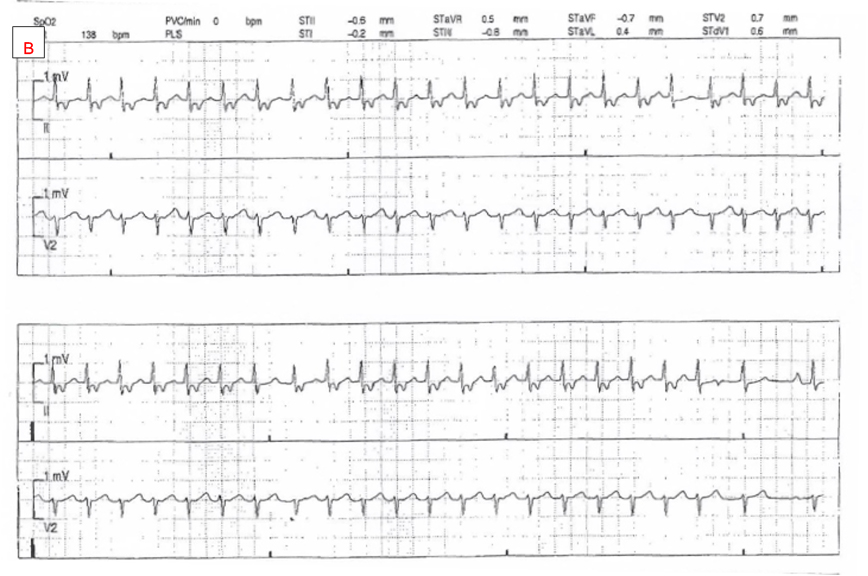
Panel B shows the rate of SVT has slowed to approximately 140bpm. All 12 leads are no longer available for P wave morphology analysis but the P wave appears unchanged in lead II. Notice that the RP interval is unchanged despite the slower tachycardia rate. Towards the end of the panel, we see a cycle where there is a dropped P wave (purple circle in between red arrows highlighting P waves). This phenomenon is seen again further along in the bottom of the panel. Tachycardia continues without reset despite the dropped P wave. This implies that atrial depolarization is not an obligate component of the tachycardia mechanism and thus option a) orthodromic AV reentry tachycardia can be excluded. This is because orthodromic AV reentry is due to the presence of a large loop circuit comprised of AV node, His-Purkinje system, ventricular myocardium, retrograde conduction to the atrium via an AV bypass tract, atrial myocardium, and then finally, the AV node again. Tachycardia is interrupted if any of these structures fail to depolarize. The dropped P waves seen here exclude orthodromic reentry because tachycardia continues at the same rate and is unaffected by the lack of atrial depolarization.
Additionally, it is readily apparent that with the dropped P waves the overall atrial rate is now lower than the ventricular rate. Consequently, the atrium cannot be driving this narrow complex tachycardia, hence options c) focal atrial tachycardia, and d) slow atrial flutter, can be excluded.
This leaves the correct answer as b) AV nodal reentrant tachycardia (AVNRT).
AVNRT is the most common form of SVT and is caused by reentrant excitation around perinodal transitional zone tissue. Neither atrial nor ventricular myocardium is required for ongoing AVNRT. While conduction block to the ventricle is commonly seen during AVNRT, block to the atrium is rarer. When conduction block to the atrium is seen during a narrow complex tachycardia however, it is very useful as it excludes most other common SVT mechanisms.
Provided by A/Prof Haris M. Haqqani – ECG of the Month – August 2022