A 16 year old girl with a history of recurrent paroxysmal palpitations and a structurally normal heart has the following 12-lead ECG recorded during an especially severe episode for which she obtained urgent medical assistance.
Which of the following is the correct diagnosis?
a) Ventricular tachycardia
b) Antidromic AV reentrant tachycardia
c) Preexcited atrial flutter
d) Orthodromic AV reentrant tachycardia with aberrance
e) AV nodal reentry tachycardia with aberrance
Explanation:
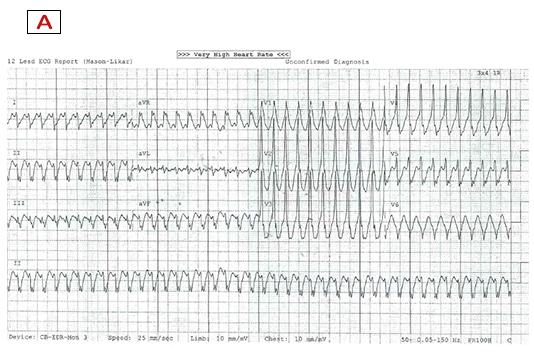
Panel A displays a very rapid, regular broad complex tachycardia at 250bpm. The differential diagnosis includes (i) ventricular tachycardia (VT), (ii) supraventricular tachycardia (SVT) with aberrance, and (iii) preexcited tachycardia. Note that (ii) is a two-part diagnosis i.e. it requires the presence of SVT along with aberrance, as without aberrance, SVT presents as a narrow complex tachycardia.
The term ‘aberrance’ conventionally refers to a functional block or delay in the bundle branches during tachycardia but which is not present in sinus rhythm. Functional bundle branch blocks display similar QRS morphology to fixed bundle branch blocks. Consequently, morphology criteria consistent with a typical right or left bundle branch block should be present to diagnose SVT with aberrance as the mechanism of any broad complex tachycardia.
In Panel A, we see a monophasic R in V1 (rather than the typical rsR’ of a right bundle branch block) and a QS in V6 (rather than the typical Rs or rS). It is axiomatic that the presence of a QS pattern in V6 is strong evidence against aberrance as no combination of bundle branch or fascicular blocks can cause wavefront propagation to proceed entirely away from the normally latest activating posterolateral left ventricular region that is closest to V6. Thus the QRS morphology is not consistent with aberrance and hence d) and e) can be excluded.
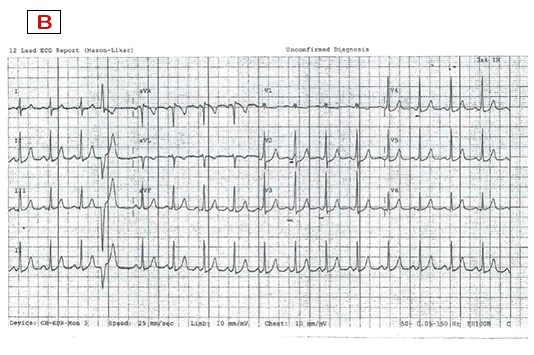
Panel B shows preexcitation in sinus rhythm with a short PR interval and delta waves. Combined with presence of symptomatic tachycardia, this establishes the diagnosis of Wolf-Parkinson-White syndrome. The positive delta wave and QRS in lead V1 and the inferior limb leads suggests the presence of a left lateral bypass tract with a ventricular insertion into the anterolateral (or superolateral) mitral annulus.
Both b) and c) are forms of preexcited tachycardia. This collection of tachycardias is defined by the presence of any antegrade (atrial to ventricular) conduction over a manifest bypass tract (accessory pathway) during broad complex tachycardia. This term is not mechanism specific and refers to a group of rhythms that exhibit at least some degree of preexcitation during tachycardia. Of these, only b) antidromic AV reentrant tachycardia exhibits ventricular activation entirely and solely over the bypass tract. This is because the AV conduction system is used retrogradely for activation of the atrium before reentry back to the ventricle over the bypass tract. As a result no antegrade conduction can occur over the AV conduction system during antidromic reentrant tachycardia.
It should be noted that, from the perspective of the ventricle, antidromic tachycardia is indistinguishable from option a) above, namely a focal ventricular tachycardia arising from a point source at the AV annulus. Such idiopathic ventricular tachycardias occur in structurally normal hearts.
Closer examination of the QRS morphology during tachycardia reveals a sharp intrinsicoid deflection in a number of limb leads and V5, in addition to a delta wave-like morphology with slurry initial forces across the majority of the precordial leads. This overall appearance is inconsistent with ventricular activation solely over a left lateral bypass tract (as it does in antidromic AV reentry tachycardia) or solely from a point source origin at the annulus (as it does in focal ventricular tachycardia). On the contrary, it implies that fusion is occurring in the ventricle with wavefront contributions from the both the bypass tract and AV conduction system during each cycle of tachycardia. Options a) and b) can thus also be excluded leaving c) preexcited atrial flutter (also known as atrial flutter with bystander preexcitation).
The diagnosis is also supported by the rapid rate and subtle suggestion of typical flutter waves in the inferior leads. This patient’s young and otherwise healthy AV conduction system was able to conduct atrial flutter 1:1 to the ventricle as evidenced by the constant fusion in each QRS with conduction over the bypass tract.
This case highlights the importance of detailed and accurate QRS morphology assessment in diagnosing the mechanism of broad complex tachycardias.
An uncomplicated catheter ablation of the left lateral bypass tract was performed and she has had no recurrence of tachycardia or preexcitation at 1 year follow up.
The Answer: c) Preexcited atrial flutter