Extensive pulmonary artery embolisation and pulmonary hypertension caused by cardiac hydatid cyst rupture
Dr Jason Harmer
This case is a rare example of cardiac hydatidosis found in a patient in rural NSW, Australia. He was a middle-aged man who initially presented with a ruptured right ventricular hydatid cyst causing an anaphylactoid-like reaction, pulmonary emboli and widespread dissemination of hydatid echinococcus throughout the lung. He survived the cyst rupture and underwent cardiac surgery, but had incomplete resection and experienced progressive cardiopulmonary hydatidosis despite ongoing antihelminthic therapy. He had an array of cardiopulmonary sequelae over his lifespan, including worsening pulmonary hypertension and right heart failure, as well as bone marrow suppression and neutropenic sepsis. This case highlights rare clinical manifestations of cardiac hydatidosis and potential complications of its treatment.
Hydatidosis is caused by ingestion of larvae from the Echinococcus granulosus tapeworm from contaminated food or water supply or by direct contact with infected animals. Hydatid cysts commonly affect the liver or lung; however, cardiac involvement can occur in rare cases (i.e. <2% of all cases of hydatidosis).
Figure 1
Transthoracic echocardiogram: apical 4 chamber view. Intracardiac hydatid cyst.
Apical attachment of a large hydatid cyst to the wall of the RV. The RV chamber is dilated and hypokinetic and the septum is dyskinetic. The distal portion of the hydatid cyst is mobile. The RA is severely dilated and the interatrial septum is displaced due to pressure overload. The tricuspid annulus appears dilated.
Figure 2
Transthoracic echocardiogram: parasternal short axis view. Intracardiac hydatid cyst.
There is a large mass (hydatid cyst) in the RV that appears to be fixed to parts of the interventricular septum. Motion of the interventricular septum is abnormal, in part due to attachment of the mass and from raised pressures in the right heart. Interventricular septal flattening is a sign of raised right heart pressures. This patient has known moderate to severe pulmonary hypertension as a consequence of dissemination of hydatid disease to the lung and pulmonary thromboembolism.
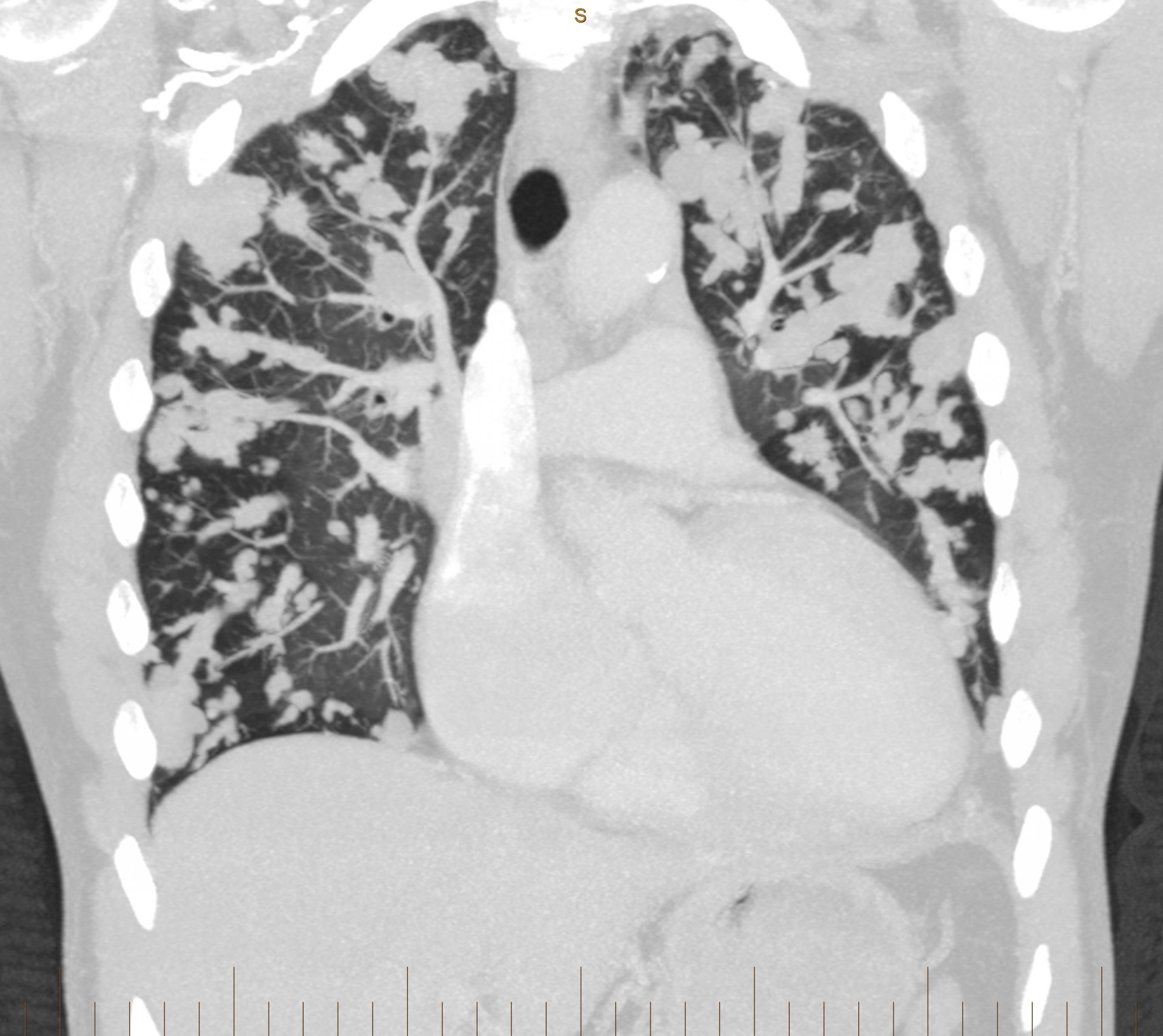
Figure 3
CT pulmonary angiogram: coronal view. Multiple hydatid masses within the pulmonary vasculature.
Multiple lobulated areas within the pulmonary vasculature from extensive dissemination of hydatid disease originating from the RV.
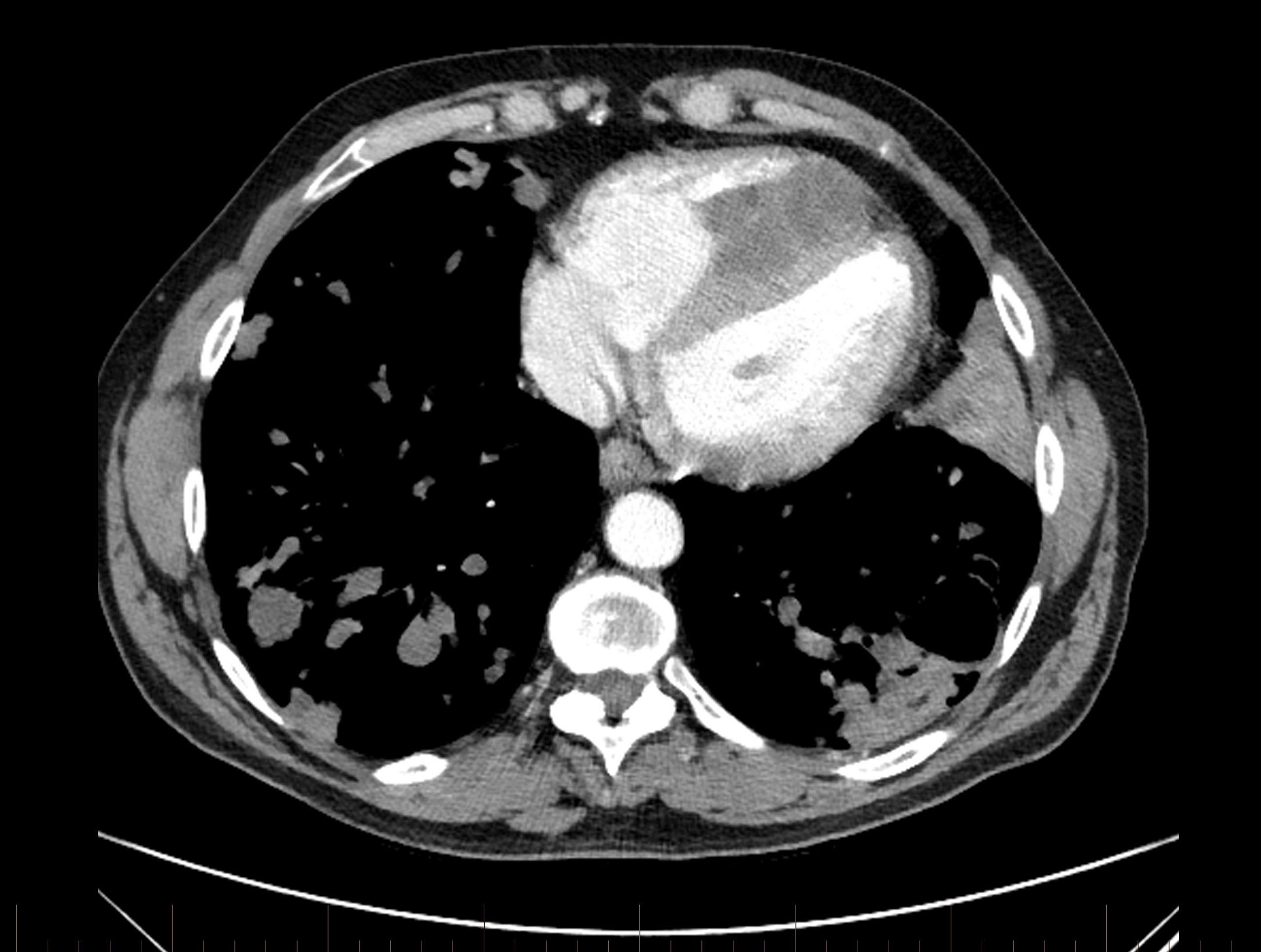
Figure 4
CT pulmonary angiogram: axial view.
There is a dense mass within the RV chamber due to a hydatid cyst. There is reduced RV blood filling in diastole due to the space occupying mass. The interventricular septal wall is clearly demarcated and the mass appears to encroach on the septal wall at two points. The RV is enlarged and occupies the apex of the heart. The sternum has been divided in two parts from a previous stenotomy (with incomplete surgical resection of the mass, leading to regrowth). There is a cavitating lesion in the posterior aspect of the left lung.
Abbrev. CT = computed tomography; RV = right ventricle; LV = left ventricle; RA = right atrium.