 Life without a pulse – LVAD emergencies.
Life without a pulse – LVAD emergencies.
Presented by Dr Felicity Lee and Chaired by Dr Nestor Gahungu.
(Viewing time approx 56 mins with Q&A)
Echocardiography for valve disease in the era of structural heart interventions
Presented by A/Prof Mayooran Namasivayam, St Vincent’s Sydney
Chaired by Dr Philip Lo
(approx viewing time: 52 mins)
Approach to management of Atrial Arrhythmia

Presented by Dr Pradyot Saklani, Sir Charles Gairdner Hospital, Perth, WA Chaired by Dr Aindreas Dorai-Raj.
(viewing time approx 1hr:05min)
Watch the presentation on Primary Prevention here by Prof Tony Stanton
(approx viewing time 1:05 hrs)
CT for structural heart disease assessment
Presented by Dr Abdul Ihdayhid
(Approx viewing time is 1 hr)
SCCT: The Role of CT for non coronary artery assessment – case based learning
Presented by A/Prof Arun Dahiya and chaired by A/Prof Dennis Wong
(Approx viewing time with Q&A 55 mins)
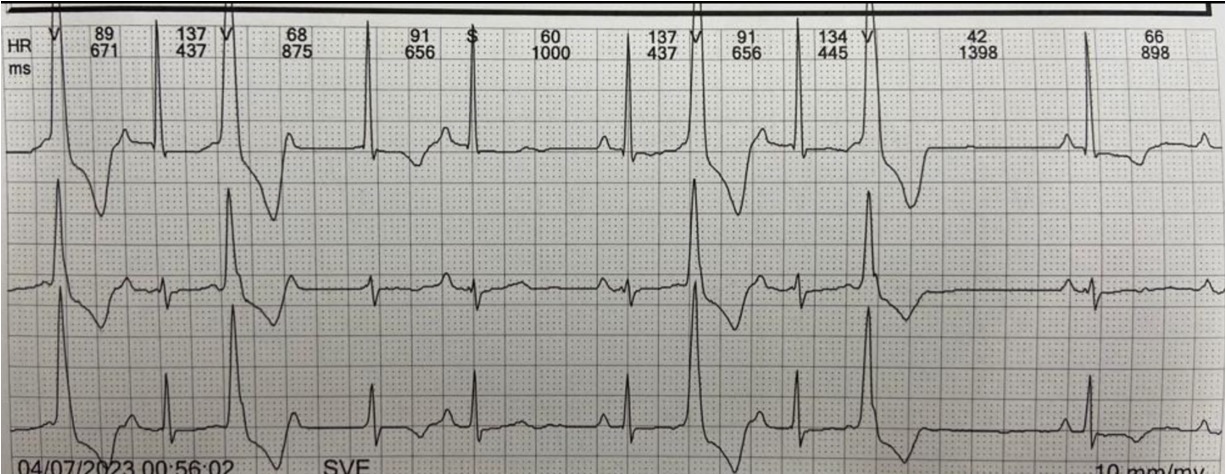
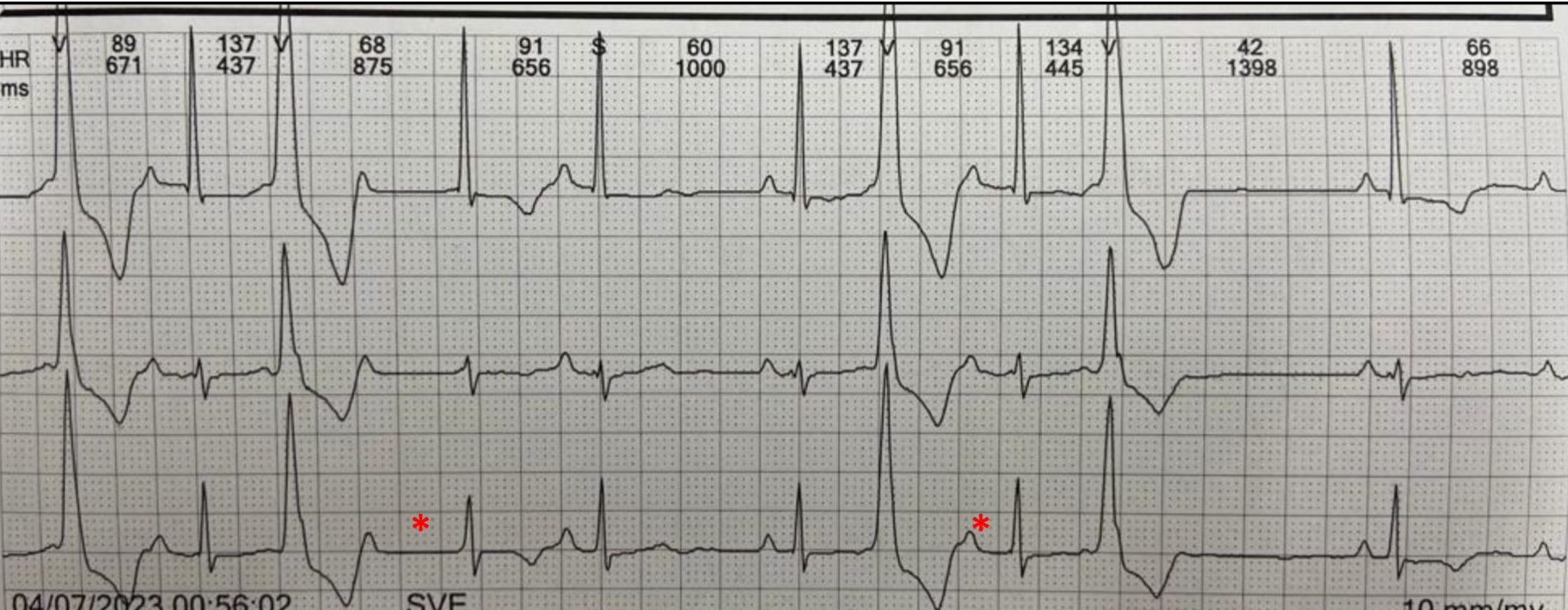
 Approach to SVT
Approach to SVT
Presented by A/Prof Alex Voskoboinik and chaired by Dr Louise Segan.

(Viewing time approx. 55 mins)
Presented by Dr Andrew Lin, (Monash Medical Centre)
Chairs: Prof Barry Elison, Dr Ryan Shulman.
(Viewing time is approximately 56 mins)
Plaque Imaging and Functional Assessment of Coronary Artery Stenosis,
Presented by A/Prof Dennis Wong, Monash Heart.
Viewing time is approximately 64 mins
 Dr Zhaleh Ataei
Dr Zhaleh Ataei