Potential for shocks to be ~79% of the programmed energy as a result of a safety feature, Short Circuit Protection, designed to truncate delivered energy to protect the device when unexpected current is detected during HV therapy.
ANZCDACC Hazard Alert June 2022
Device:
Medtronic Cobalt XT™, Cobalt™ and Crome™ Implantable Cardioverter Defibrillators (ICDs) and Cardiac Resynchronisation Therapy Defibrillators (CRT-Ds)
TGA Reference: RC-2022-RN-00811-1
Australian Register of Therapeutic Goods (ARTG):
339481, 339482, 339483, 339484, 339485, 339486, 339487, 339488, 339489, 339490, 339491, 339492, 341547, 341548, 341549, 341551, 341552, 341555, 341556, 341557, 341558, 341553, 341550, 341554
Advisory grade TGA: Class I
(Class I recall action occurs when the product deficiency is potentially life-threatening or could cause a serious risk of health).
Description:
In the case where a forementioned ICD/CRTD determines a high-voltage (HV) therapy shock is necessary, there is a potential for this shock to be only ~79% of the programmed energy.
The potential for reduced shock energy is the result of a safety feature, Short Circuit Protection (SCP), that is designed to truncate delivered energy to protect the device when unexpected current is detected during high-voltage (HV) therapy. All Cobalt/Crome devices include the SCP feature. SCP events can trigger during delivery of the HV biphasic waveform in the presence of a lead insulation breach (typically first-phase SCP) or unexpected, additional current in the device HV circuit (typically second-phase SCP).
Analysis of returned devices has confirmed Cobalt/Crome devices can be sensitive to a non-destructive, secondary current pathway involving the HV circuitry. This secondary current does not permanently impair the device’s internal circuitry or battery, but it can result in an electrical switch (that controls current flow during HV delivery) to intermittently remain active for longer than intended after delivery of the first phase of the biphasic waveform. When the secondary current flow through the active switch is detected, the SCP feature truncates delivery of the remaining HV energy.
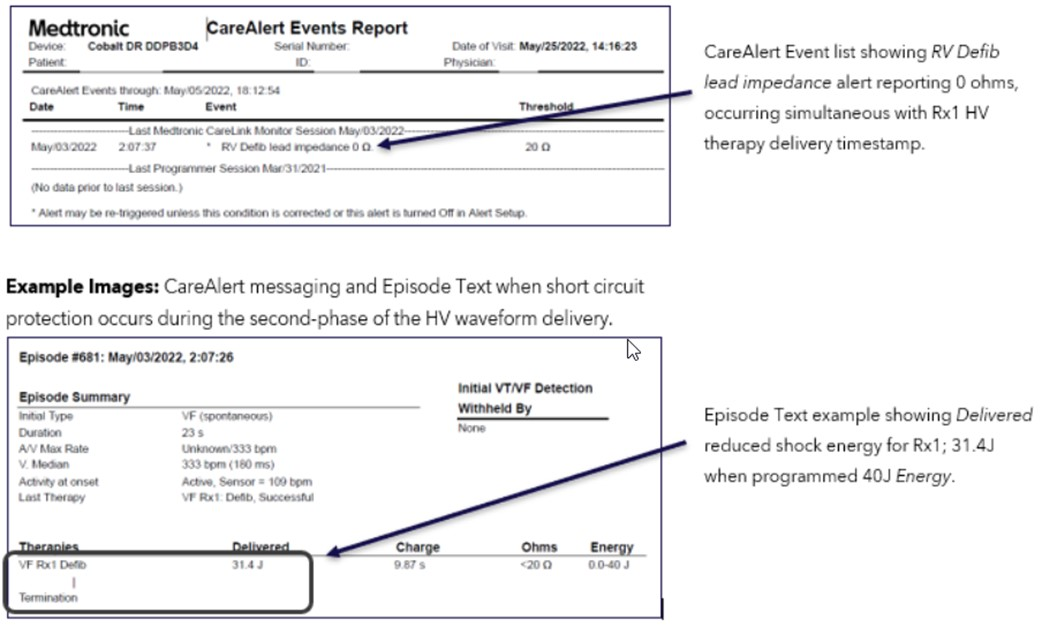
In Cobalt/Crome devices, an RV Defib lead impedance alert reporting zero (0) ohms will be displayed simultaneous with HV therapy delivery (see example images in the “Presentation” section).
After an SCP event, devices will continue to operate as programmed. Pacing, sensing, episode detection, and anti-tachycardia pacing (ATP) therapies are not impacted by a second-phase SCP event; additionally, HV charging, battery longevity and Bluetooth telemetry are not impacted.
Review of episode data from reported complaints confirms successful delivery of the first-phase energy, and that the second phase of the programmed energy is truncated. When a second-phase SCP event occurs, ~79% of the programmed output is delivered as a monophasic waveform.
Although not observed clinically, HV therapy programmed to the AX>B configuration, or any configuration with Active Can/SVC Coil set to “Can Off,” creates the potential for residual current to flow back to the heart, theoretically resulting in proarrhythmia. Medtronic has confirmed the B>AX configuration (with Active Can On) mitigates the risk for proarrhythmia from this unintended current flow.
Additional analysis has confirmed the switch-mechanism can be intermittent, resulting in HV therapy sequences delivering both the intended full-energy biphasic waveform and/or a reduced-energy monophasic waveform within the same therapy episode. Therefore, programming a 40J output provides the best opportunity to deliver the highest shock energy if the device experiences a second-phase SCP event: in this case, a 32J monophasic waveform will be delivered.
Medtronic has submitted a device software update to address this issue and anticipates it will be available for download into implanted devices beginning third/fourth quarter of calendar year 2022. The update will ensure the full shock energy is delivered in the presence of a secondary, low-level current pathway in the HV circuitry.
Medtronic has not received any reports of permanent harm or death due to this issue.
Based on analysis of peer-reviewed literature as well as CareLink data on shock efficacy from more than 279,000 episodes (Medtronic data on file, May 2022), termination success rates for 32J (~79% of 40J), monophasic shocks versus 40J biphasic shocks are estimated in Table 1. Termination success may vary depending on individual patient risk factors and medication use.
Table 1
| Normal operation (40J, Biphasic energy) | Second-phase SCP (32J, Monophasic delivery) | |
| Estimated First Shock Success* (in VF zone) | 89% | 85% |
| Estimated Cumulative Success Shocks 1-6* | 99% | 98% |
Potential harms related to a second-phase SCP event include failure to terminate the arrhythmia due to reduced-delivered-energy, a theoretical risk of proarrhythmia, and complications associated with device replacement, including unnecessary lead replacement due to misinterpretation of the SCP alert.
- While not observed clinically, Medtronic estimates the risk for proarrhythmia is 0.002% in the AX>B configuration, and improbable in the B>AX configuration (less than 0.00004%), with Active Can pathway enabled. These risks may be higher when Active Can is disabled.
- The overall risk for patient mortality due to this issue is estimated to be 0.002% at 24 months when combining the likelihood, a patient will need therapy with the probability an arrhythmia fails to terminate after six sequences of 32J monophasic shocks.
- Comparatively, the risk of patient mortality due to complications associated with device replacement is 0.032% -0.043% 1,2,3.
Number of devices affected in Australia and New Zealand:
2979
Presentation:
When a Short Circuit Protection (SCP) event occurs, Cobalt/Crome devices will;
- Issue an RV Defib lead impedance alert reporting zero (0) ohms that occurs simultaneous with HV therapy delivery (see example images below).
a. A fixed value of zero (0) ohms indicates that a short circuit was detected during HV therapy delivery. - Display the delivered energy of the episode as ~79% of the programmed energy (eg. 31.4J when programmed to 40J).
As a result of the reduced energy delivery, patients are more likely to present with failed and multiple shocks.
Rate of occurrence:
Through 03 June 2022, Medtronic has identified 27 devices (0.03% of devices distributed worldwide) that have experienced a reduced-energy shock, which is accompanied by a Short Circuit Protection (SCP) alert.
While 0.03% has been observed to date, Medtronic projects 0.18% of the ~80,000 distributed devices may experience a second-phase SCP within 24 months of service life, when considering the probability for these SCP events increases overtime, and the likelihood a patient will need HV therapy during that time.
- For the population of patients who received HV therapy, the observed rate was 0.77%. When projecting for this population, the chance of encountering a second-phase SCP event is ~5.0% at 24 months.
Note: The above projections are based on calculations without the planned device software update. Once installed, this update, in addition to the programming recommendations, will resolve occurrences of second-phase SCP events.
Recommendation:
Each patient requires unique clinical considerations.
- Until the software update is available, carefully consider the risks versus the benefits of implanting a Medtronic Cobalt XT™, Cobalt™ or Crome™ ICD or CRTD.
- Prophylactic device replacement is not recommended.
- Patients programming should be assessed and, if necessary, have their next regularly scheduled follow-up conducted in person to allow for device reprogramming
a. Consider programming all HV therapy Energy to 40J and Pathway settings to B>AX and Active Can/SVC Coil set with Active Can enabled across all therapy zones.
b. If the “Get Nominals” feature is used, be aware that AX>B is set pending for Rx5 and Rx6 and should be reprogrammed B>AX.
c. If a patient requires Active Can be programmed Off, contact Medtronic Technical Services for further guidance.
d. Ensure the RV Defib Lead Impedance Out of Range alert is enabled (this alert is shipped On with both Device Tone and Wireless CareAlert enabled). - Remind patients to contact the clinic if they hear an audible tone coming from their device.
- Remind patients to keep their home monitor plugged in at all times, or their MyCareLinkHeart™ smartphone app open and active in the background at all times.
- For patients in whom high DFT is suspected, consider DFT testing to ensure a 10J safety margin exists.
a. For manually delivered shocks, no episode data is stored, and no CareAlerts are triggered; Review Last HV Therapy values displayed on the Battery and Lead Measurement screen (Data >>Battery and Lead Measurements) to determine if a reduced-energy shock was delivered. If a second-phase SCP occurs during DFT delivery, the device will display ~32J for a 40J programmed output.
b. Successful delivery of full-energy shocks during manual delivery does not guarantee future delivery of full-energy shocks for spontaneous arrhythmias. - If an RV Defib lead impedance alert reporting zero (0) ohms is observed, this is evidence that an SCP event has occurred. Contact Your Local Medtronic Representative for confirmation on the source of the impedance alert.
a. A Save-Session file or a CareLink transmission file will be requested; Medtronic Technical Services can use stored device information to confirm whether the SCP event is due to a suspected lead issue, or due to unexpected current in the HV circuit.
b. If the delivered energy during the episode is ~79% of the programmed energy AND the SCP alert indicates an RV Defib Lead impedance alert reporting exactly zero (0) ohms, this is an indication of a second-phase SCP event and not a lead issue. - After confirming the cause of the RV Defib Lead Impedance alert with Medtronic Technical Services:
a. Consider device replacement commensurate with the patient’s underlying health and history, with the understanding a device has an ~81% probability of delivering subsequent reduced-energy shocks, and with the understanding an update for implanted devices is anticipated to be available beginning third quarter/fourth quarter of calendar year 2022.
b. If the device remains implanted, ensure all HV therapy sequences, programmed parameter settings and SVC Coil pathway (where appropriate) are as desired following any lead replacement.
References:
- Tarakji KG, et al. Antibacterial Envelope to Prevent Cardiac Implantable Device Infection. The New England Journal of Medicine. 2019;380(20):1895-1905.
- Medtronic Data on File. MDT2260884-CRHF CIED Infection Report; Agile: MDT2260884, Version 2.0, 11/02/2015.
- Birnie D, et al. Complications associated with defibrillation threshold testing: The Canadian experience. Heart Rhythm. 2008; 5(3):387-90.
The ANZCDACC encourage you to report any adverse event or near (potential) adverse event associated with the use of a medical device including any abnormal CIED or lead function. We encourage reporting to ANZCDACC directly via the Committee chair Dr Paul Gould [email protected] and to the following regulators.
In Australia, report to the TGA;
| Online | https://www.tga.gov.au/reporting-problems |
In New Zealand, report to Medsafe;
| Post | Compliance Management Branch, Medsafe, PO Box 5013, Wellington 6145. |
| [email protected] | |
| Fax | 04 819 6806 |