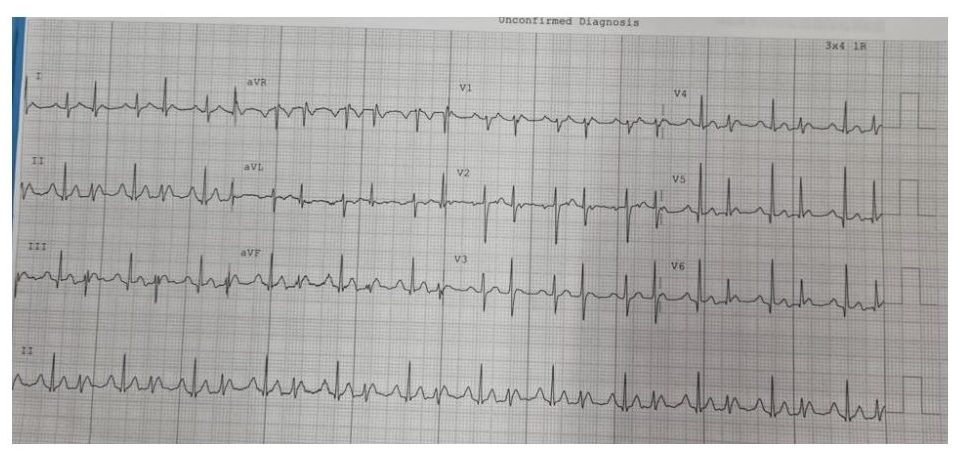
A 25 year-old male with no past history presents with palpitations.
What is the most likely diagnosis? Why are there two QRS morphologies?
The Answer:
This is a ‘regularly irregular’ narrow complex tachycardia (hence not AF). There are clear p-waves marching through (with more A’s than V’s) with an isoelectric interval between them suggestive of a focal atrial tachycardia (blue arrow), particularly in the absence of structural heart disease. The p waves are inferiorly directed, suggesting they are coming from the top of the atria. In this case, there is Wenckebach conduction down the AV node (3:2 ratio) with progressive PR prolongation before a dropped beat. The change in QRS morphology is due to Ashman phenomenon – this is aberrant ventricular conduction affecting the distal conduction system due to a change in QRS cycle length, and it can be seen in any supraventricular arrhythmia. It is usually described as a wide QRS complex that follows a short R-R interval preceded by a long R-R interval (L – long, S – short in Figure). I occurs because the action potential duration (and hence refractory period) changes with the preceding R–R interval. A longer cycle lengthens the ensuing refractory period, and if a shorter cycle follows, the beat terminating the cycle tends to be conducted with aberrancy. The patient underwent catheter ablation of a focal tachycardia arising near the crista terminalis / SVC region.
