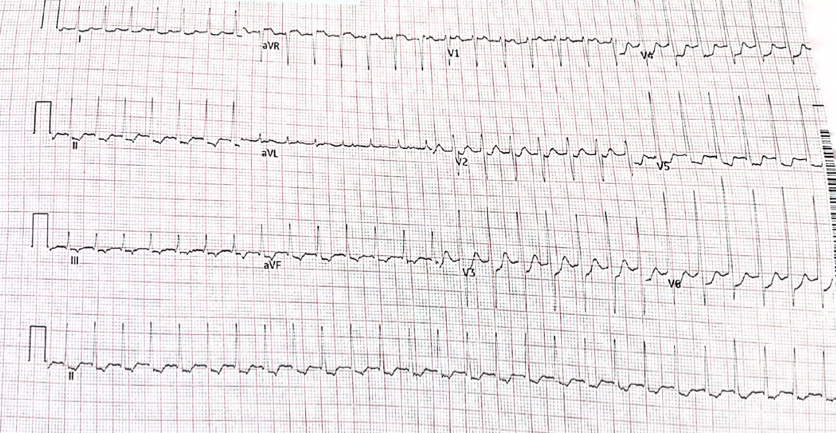
A 72 year old woman presents with palpitations and pre-syncope. Initial ECGs is shown below (Figure 1):
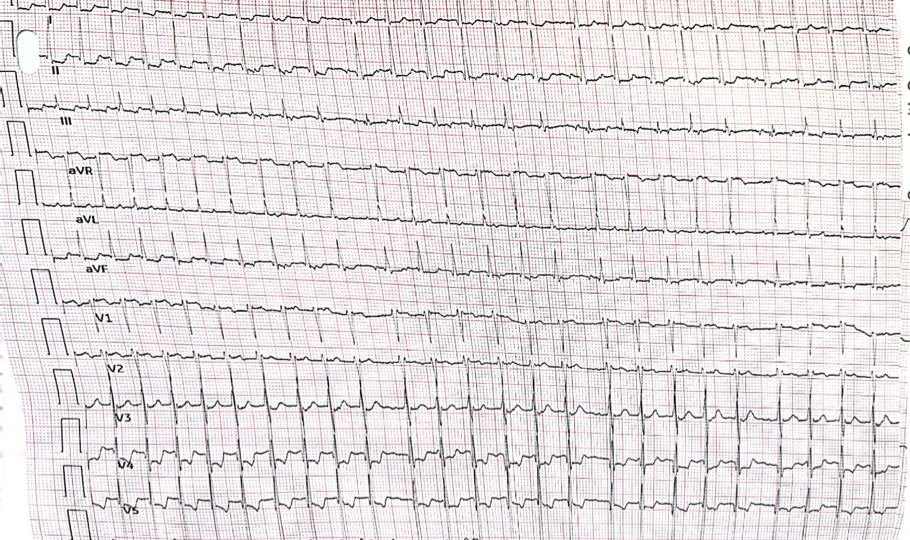
A Valsalva manoeuvre is attempted and subsequent ECG is shown below (Figure 2):
What is the most likely diagnosis? Want to ask a question or discuss visit the ECG Forum…
Answer:
Atrial tachycardia with Wenckebach AV nodal conduction.
Explanation:
The initial ECG demonstrates a ‘short RP’ SVT with the p-wave best seen in lead aVL on the initial ECG. The differentials are typical atrioventricular nodal reentrant tachycardia (usually the retrograde p wave is buried at the end of the QRS which is not the case here), atrioventricular reentrant tachycardia or atrial tachycardia (AT) with first degree AV block.
The second ECG following a ‘vagal’ manoeuvre does not terminate the tachycardia but increases the block at the level of the AV node. This exposes the p-waves and there are more ‘A’s than ‘V’s with grouped beating seen (best appreciated in lead III). This Wenckebach pattern excludes AVRT (in fact by definition the A:V relationship must be 1:1) and makes AVNRT very unlikely. The p-wave morphology is nearly isoelectric in V1 and very ‘skinny’ suggesting a mid-line origin. In pact at EP study the focal atrial tachycardia was mapped to the perinodal region and successfully ablated there.