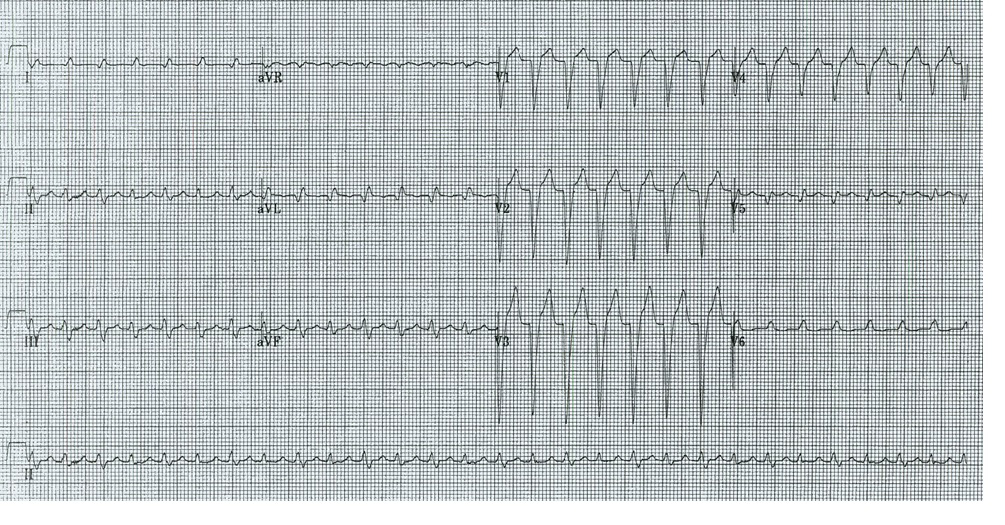
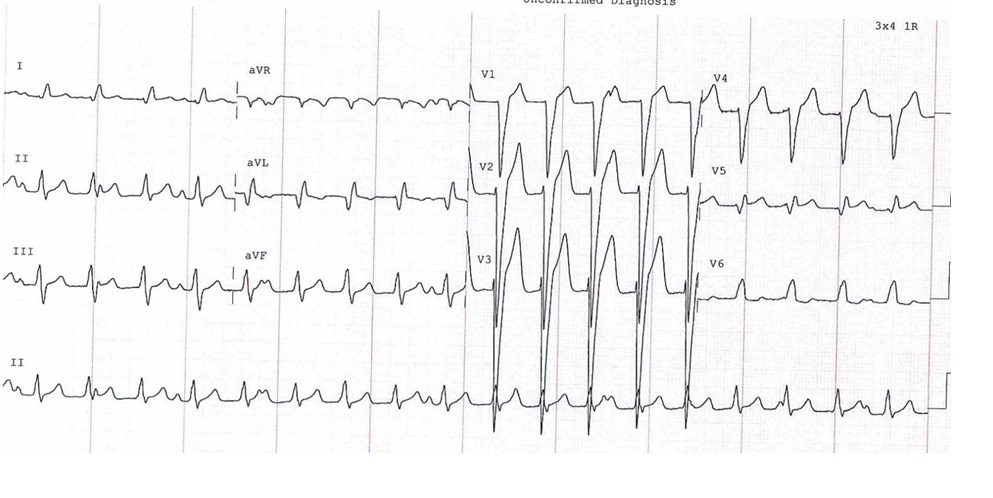
Stem: A 29 year-old male presents with a 2 month history of frequent palpitations. His initial ECG is shown in Figure A. Bedside TTE shows mild-moderate global LV dysfunction. What are the differential diagnoses?
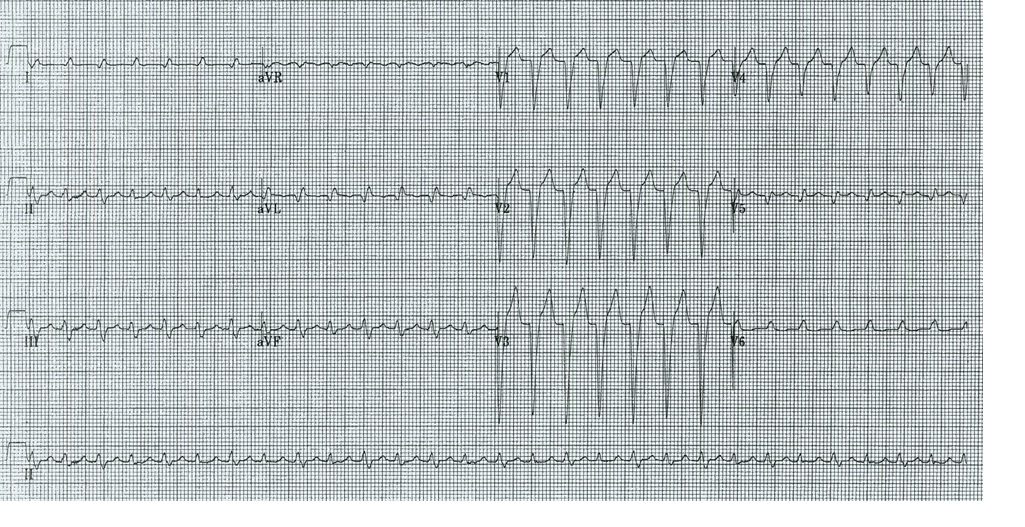
Answer: This is a regular wide complex tachycardia with left bundle branch block morphology (QRS width ~ 125ms). Differential diagnoses for regular wide complex tachycardia (QRS > 120 ms) in general include VT, SVT with aberrancy (any regular SVT – inc. atrial tachycardia, AVNRT, AVRT, atrial flutter, sinus tachycardia), and pre-excited tachycardia. The typical LBBB morphology suggests that the ventricle is being activated from the region of the right bundle. Hence, specific diagnoses to consider given the morphology include SVT with LBBB aberrancy (or fixed LBBB), bundle branch reentrant VT, idiopathic moderator band VT and atriofascicular antidromic tachycardia.
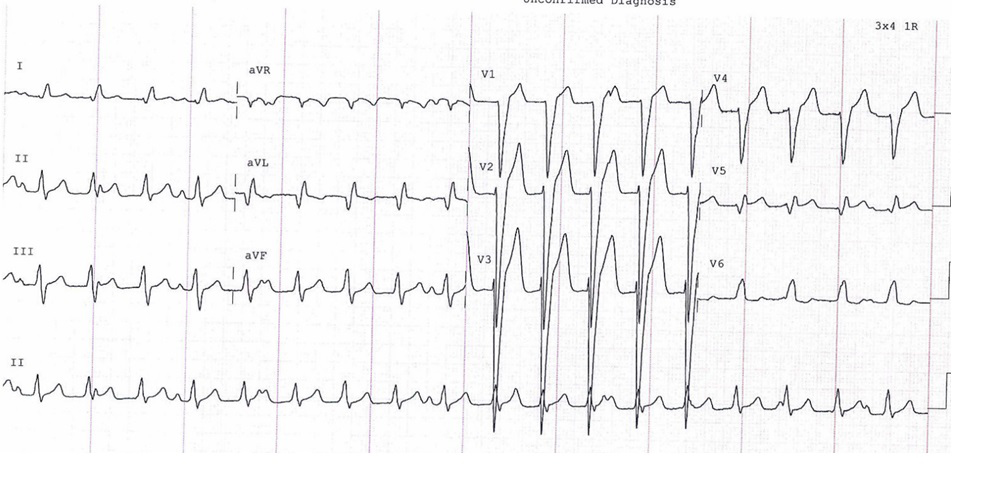
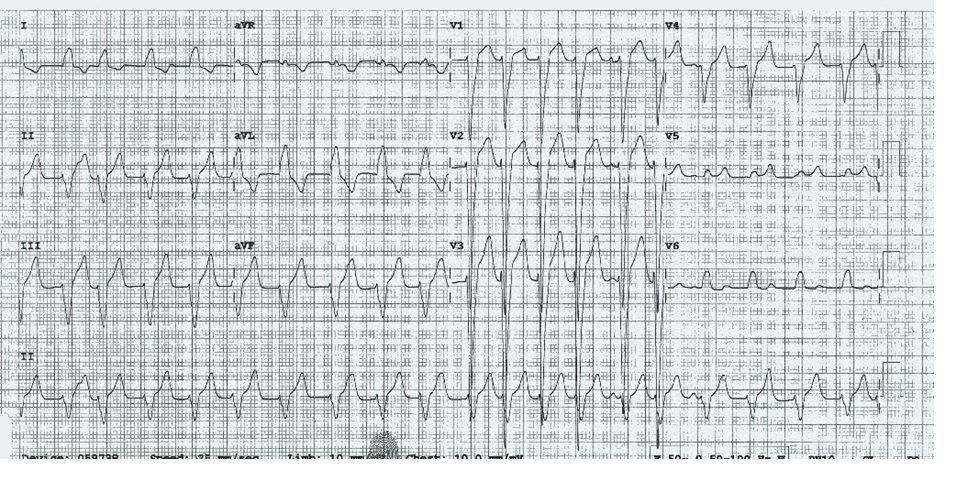
Stem (continued): Adenosine was given with no effect suggesting this was less likely to be a re-entrant SVT involving the AV node (ie. AVNRT, AVRT). He was subsequently given metoprolol and amiodarone – ECGs post are shown (Figure B and C). Does this help with the diagnosis?
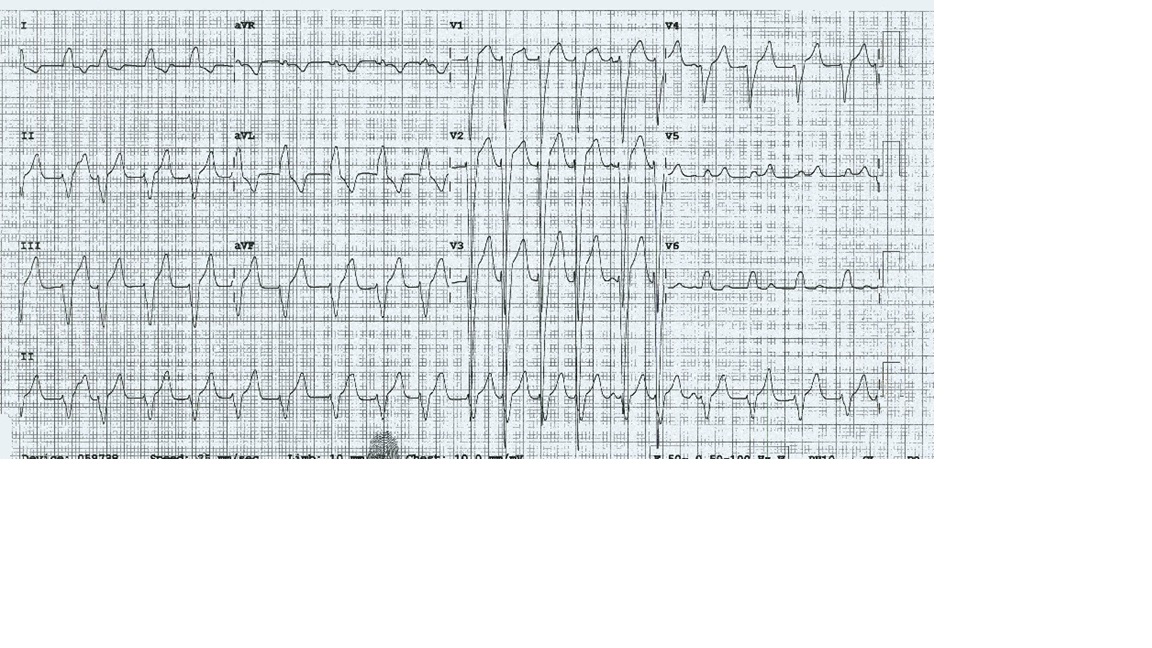
Answer: These ECGs rule in VT – there is clear cut AV dissociation (sinus p waves regularly marching through). In Figure C, there is some irregularity suggesting an automatic (rather than re-entrant) mechanism. VT continued despite cardioversion and amiodarone. Thus the patient has incessant VT causing a tachycardia mediated cardiomyopathy. Catheter ablation was performed with the focal VT successfully ablated at the moderator band (adjacent to the exit of the right bundle – hence the typical LBBB morphology). LV function returned to normal after 2 months.
Want to discuss these further – Ask a Question of A/Prof Alex Voskoboinik or upload your own Images for discussion.
Uploaded files: