Guideline-Directed Medical Therapy Before and After Primary Prevention Implantable Cardioverter Defibrillator Implantation in New Zealand (ANZACS-QI 66)
Authors: Fang Shawn Foo, MBChB; Mildred Lee, MSc; Katrina K. Poppe, PhD; Geoffrey C. Clare, MBChB; Martin K. Stiles, PhD; Andrew Gavin, MBChB; Matthew Webber, MBChB; Rod Jackson, PhD; Andrew J. Kerr, MD;
Published in Heart Lung and Circulation 20 August 2022 with summary below by Dr Shawn Foo and A/Prof Martin Stiles.
Patients with heart failure and reduced ejection fraction are recommended to receive guideline directed medical therapy (GDMT). Many of these patients will also receive an ICD. This prompted Foo et al to look at almost 1700 ICD patients in New Zealand and, using prescribing records, determine which of these patients were receiving such medications at implant and one year later, and whether target doses were achieved. The specific classes of medication assessed were:
1. ACEi/ARB/ARNI
2. Beta blockers
3. Aldosterone antagonists
Note that the study period of 2009-2018 pre-dated the use of SGLT2 inhibitors.
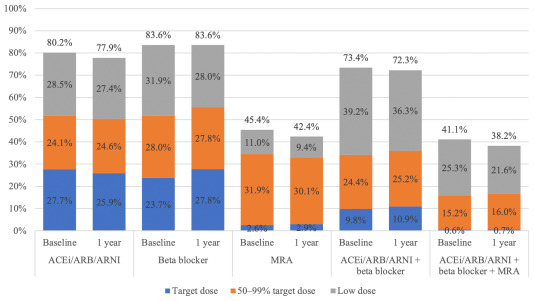
Foo found that although 80% of patients received ACEi/ARB/ARNI, 84% beta blockers and 45% aldosterone antagonists, a dose ≥50% of recommended target dose (based on international guidelines) was achieved in only 52%, 52% and 35%, respectively. In fact, just 16% of patients received ≥50% of the target dose of all three medication classes.
For the >98% of ICD recipients who were alive at one year, the proportions of patients dispensed each class of medication remained largely unchanged. In fact, no matter the class of medication, the vast majority (67-81%) of patients had no change to their medication dose between implant and one year later.
This data is important as it captures an entire nation through its national database and demonstrates the inertia of heart failure therapy. This group of ambulatory heart failure patients would likely benefit from a more intensive up-titration of medication doses to ensurethat the (now four) classes of GDMT were all prescribed, where appropriate.
Some of the patients in this cohort would have been at maximally-tolerated doses yet not achieved ≥50% of the recommended target dose due to limitations of (e.g.) low blood pressure or kidney function, but there is clearly room for improvement. Perhaps a greater integrated response from ICD clinics and heart failure services would improve the numbers of patients at target dose, translating to improved outcomes in such endpoints as hospitalisations and mortality. In fact, some have argued that repeating the primary prophylactic ICD trials in today’s era of four-agent heart failure therapy might demonstratelack of benefit for ICDs over modern medical therapy. This study suggests that, until we do better in replicating the doses achieved in pivotal trials, medical therapy for heart failure in practice does not match ‘gold-standard’ GDMT of the trials.
Guideline-directed medical therapy for heart failure in patients before and after receiving primary prevention ICD implant 2009-2018.
Abbreviations: ACEi, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blockers; ARNI, angiotensin receptor neprilysin inhibitors; ICD, implantable cardioverter defibrillator; MRA, mineralocorticoid receptor antagonists.
Published: August 20, 2022. DOI:https://doi.org/10.1016/j.hlc.2022.06.691