Presented by Dr Seshika Ratwatte
Pulmonary hypertension (PHT) commonly co-exists with significant mitral regurgitation (MR), but its prevalence and prognostic importance has not been well documented. In MR, PHT is thought to be due to the direct effect of systolic backflow into the left atrium (LA), causing backpressure into the pulmonary vasculature and may develop before patients experience symptoms or left ventricular (LV) systolic dysfunction.
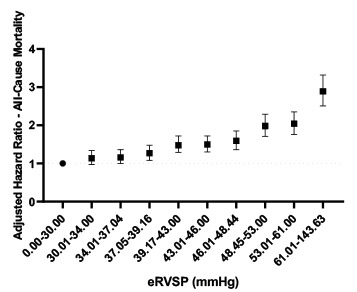
In an upcoming publication in Open Heart, Dr Seshika Ratwatte, senior author Professor David Celermajer and their co-authors identify a cohort of 9683 patients with “isolated” moderate or severe MR and preserved left ventricular ejection fraction (LVEF>50%) using the National Echo Database of Australia (NEDA). The authors show that the risk of all-cause mortality progressively increases as eRVSP level increases even after adjustment for age and sex, with an ‘inflection’ for mortality seen from eRVSP 34mmHg onwards (Central Illustration).
The publication confirms the high prevalence of PHT in patients with significant MR and preserved LVEF on echo (59.6%). Whilst a treatment effect was not reported, it was demonstrated that even minor elevations in pulmonary pressures were associated with negative prognostic implications. Consistent with the authors work on PHT in aortic regurgitation a typical phenotype of “left heart disease” on echo was confirmed the proportion of patients with RV dilation and functional impairments as well as right and left atrial sizes increasing progressively, from no PHT to severe PHT.