

STUDY REVIEW Long-Term Evolocumab in Patients with Established Atherosclerotic Cardiovascular Disease: FOURIER OLE
View the Research Review’s STUDY REVIEW below, with commentary by A/Prof John Amerena:

Heart Failure Research Review, Issue 72, with commentary by Prof Andrew Coats
In this issue:
- Iron deficiency in HF
- Contemporary SGLT-2 inhibitor use in HF patients with diabetes
- Primary care HF service for identifying missed diagnoses of HFREF
- Renal dysfunction’s impact on cardiac outcomes and end-stage renal disease in HF with mitral regurgitation
- Weekend vs. weekday admissions for HF, with/without AF
- Long-term survival and life expectancy following acute HF hospitalisation
- Efficacy and safety of dapagliflozin in HF according to frailty
- Iron deficiency and anaemia in ambulatory chronic HF patients
Download Heart Failure Research Review, Issue 72, with commentary by Prof Andrew Coats

ESC (European Society of Cardiology) Congress – 2022, with commentary by Prof John French
In this edition:
- ADVOR: acetazolamide in acute HF
- REVIVED: percutaneous revascularisation for ischaemic LV dysfunction
- Genotype-guided P2Y12 inhibitors reduce ischaemic events post-PCI
- Meta-analysis of DELIVER and EMPORER-Preserved
- PACIFIC-AMI: asundexian + DAPT after acute MI
- ALL-HEART: allopurinol and CV outcomes in ischaemic heart disease
- SECURE: polypills for secondary prevention
- PERSPECTIVE: sacubitril/ valsartan and cognitive function in HF
- TIME: morning vs. evening antihypertensives
- POST-PCI: routine stress testing after high-risk PCI

Study Review: Primary prevention of CDX and Heart Failure, with commentary by Ryan G Paul
From Research Review NZ: Learn more about the primary prevention of cardiovascular and heart failure events with SGLT2 inhibitors, GLP-1 receptor agonists, and their combination in type 2 diabetes, with commentary by Ryan G Paul, Auckland NZ
Download: Study-Review-2022-Primary-prevention-of-CDX-and-Heart-Failure

Cardiology Practice Review: Issue 23, with commentary by A/Prof John Amerena
In this issue
- Cardiovascular drug interactions with Paxlovid in COVID-19
- Myocarditis: Review article
- Myocarditis following COVID-19 mRNA vaccination of adolescents in Australia
- Cardiometabolic outcomes after COVID-19 infection
- Guidelines for ventricular arrhythmias and prevention of SCD
- Management of ACS in older adults
- NAFLD and risk of new-onset HF
- ATAGI guidance on myocarditis/pericarditis after COVID-19 vaccines
- TGA – new and extended registrations
- Associations between dietary fibre and CV risk factors
- Association of gestational diabetes with CV and cerebrovascular diseases
- COVID-19 resources
- Conferences, workshops and CPD
Download the Australian Cardiology Practice Review: Issue 23 here
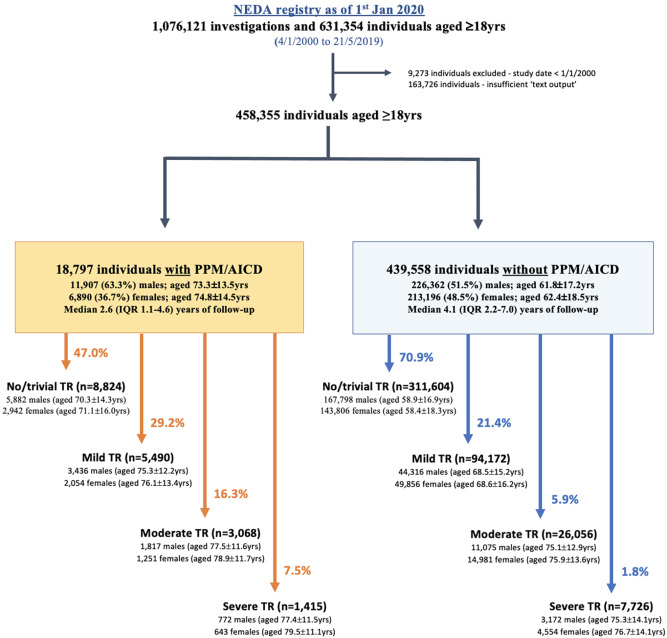
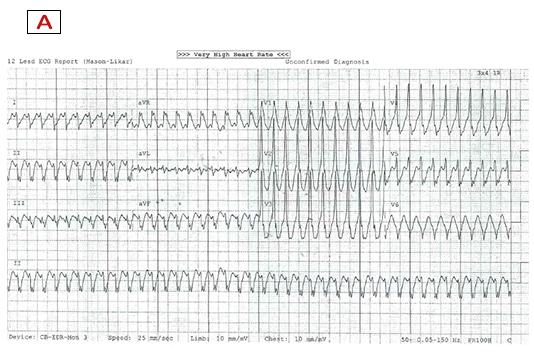
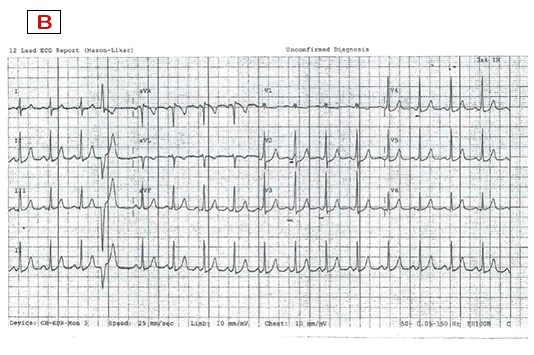
Prevalence and prognostic impact of tricuspid regurgitation in patients with cardiac implantable electronic devices
Prevalence and prognostic impact of tricuspid regurgitation in patients with cardiac implantable electronic devices: From the national echocardiography database of Australia
The prevalence and prognostic impact of tricuspid regurgitation (TR) in patients with a cardiac implantable electronic devices (CIEDs) is not well understood. This month in IJC [1] we published the results of the largest retrospective study on the subject to-date using the National Echo Database of Australia (NEDA). We found that moderate or greater TR is prevalent (23.8%) and 2-fold greater than in those without devices. Furthermore, moderate and severe CIED-associated TR was associated with a 1.6 to 2.5-fold increase in all-cause mortality. The association of CIED-related TR with a poor prognosis was also especially pertinent in younger individuals. With an ageing population and expanding indications for life-saving device-therapy, these findings highlight the need for close follow-up of patients with device therapies and for clinicians to be cognisant of the potential adverse consequences of CIED-associated TR.
Sophie Offen, Geoff Strange, David Playford, David Celermajer and Simon Stewart.
[1.] Offen S, Strange G, Playford D, Celermajer DS, Stewart S. Prevalence and prognostic impact of tricuspid regurgitation in patients with cardiac implantable electronic devices: From the national echocardiography database of Australia. International Journal of Cardiology 2022. https://www.sciencedirect.com/science/article/abs/pii/S0167527322016710


R T Hall Lecture – CSANZ 2022
The RT Hall Lecture was presented by Dr Michael J. Ackerman MD. His presentation: “Athletes with sudden cardiac death predisposing genetic heart diseases: Who says that I can’t play anyway?” was highly entertaining and very well received.
CSANZ Members can view it here R T Hall Lecture 2022